Go ahead and blame former President Clinton for calling attention to colon cancer by declaring this month National Colon Cancer Awareness Month. Back in 2000, he knew what he was doing: it’s an opportunity to spread colon cancer awareness. I know it’s not the sexiest topic, but we all need to think about our colons, especially once we hit 50.
That’s when it’s recommended you start routine screening, unless you’re at increased or high risk for colorectal cancer; then, you need to talk to your doctor about starting earlier.
You may be at increased risk if you or a close relative have had polyps or colorectal cancer; you have inflammatory bowel disease or certain genetic syndromes likeGo ahead and blame former President Clinton for calling attention to colon cancer by declaring this month National Colon Cancer Awareness Month. Back in 2000, he knew what he was doing: it’s an opportunity to spread colon cancer awareness. (FAP)or hereditary non-polyposis colorectal cancer (known as Lynch syndrome).
Some important colorectal (aka colon cancer) facts
- Colorectal cancer develops in the colon or rectum (also known as the large intestine)
- It’s the third most commonly diagnosed cancer and the third leading cause of cancer death in both men and women in the United States.
- The American Cancer Society estimated that 136,830 people would get diagnosed with colon cancer in 2014 and 50,310 would die from the disease.
What’s most important to know: you need to get screened. To me, that’s obvious. Colon cancer is one of the most preventable cancers, and screening is a way to reduce your risk. If it’s found early, colon cancer is one of the most treatable cancers.
But unfortunately, in 2010, only a little more than half of those aged 50 or older reported having screening consistent with current guidelines, according to the National Health Institute Survey. It’s estimated that if everyone 50 or older got screened regularly, up to 60 percent of deaths from colon cancer could be avoided.
What is colorectal cancer?
Colorectal cancer is a disease in which abnormal cells in the colon or rectum divide uncontrollably, ultimately forming a malignant tumor. (The colon and rectum are parts of the body’s digestive system, which takes up nutrients from food and water and stores solid waste until it passes out of the body.)
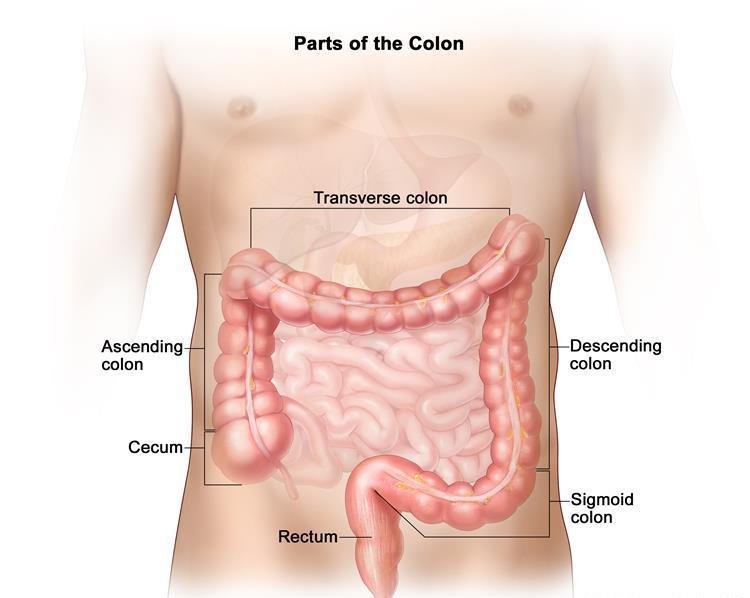
Parts of the colon. Drawing of the front of the abdomen that shows the four sections of the colon: the ascending colon, the transverse colon, the descending colon, and the sigmoid colon. Also shown are the small intestine, the cecum, and the rectum. The cecum, colon, rectum, and anal canal make up the large intestine. The cecum, ascending colon, and transverse colon make up the upper, or proximal, colon; the descending colon and sigmoid colon make up the lower, or distal, colon.
Most colorectal cancers begin as a polyp, a growth in the tissue that lines the inner surface of the colon or rectum. Polyps may be flat, or they may be raised. Raised polyps may grow on the inner surface of the colon or rectum like mushrooms without a stalk (sessile polyps), or they may grow like a mushroom with a stalk (pedunculated polyps). Polyps are common in people older than 50 years of age, and most are not cancer. However, a certain type of polyp known as an adenoma may have a higher risk of becoming a cancer.
Colorectal cancer is the third most common type of non-skin cancer in both men (after prostate cancer and lung cancer) and women (after breast cancer and lung cancer). It is the second leading cause of cancer death in the United States after lung cancer. In 2016, an estimated 134,490 people in the United States will be diagnosed with colorectal cancer and 49,190 people will die from it.
The rates of new colorectal cancer cases and deaths among adults aged 50 years or older are decreasing in this country due to an increase in screening and to changes in some risk factors (for example, a decline in smoking). However, incidence is increasing among younger adults for reasons that are not known. For example, researchers predict that by 2030, based on current U.S. trends, colon cancer incidence rates will increase by 90% for people aged 20 to 34 years and by 28% for people aged 35 to 49 years, whereas they will decrease by 38% for people aged 50 to 74 years and by 45% for those 75 years or older.
The major risk factors for colorectal cancer are a family history of the disease and older age, but several other factors have been associated with increased risk, including excessive alcohol use, obesity, being physically inactive, cigarette smoking, and, possibly, diet.
In addition, people with a history of inflammatory bowel disease (such as ulcerative colitis or Crohn disease) have a higher risk of colorectal cancer than people without such conditions. And people who have certain inherited conditions (such as Lynch syndrome and familial adenomatous polyposis ) also have an increased risk of colorectal cancer.
Several screening tests have been developed to help doctors find colorectal cancer early, when it may be more treatable. Some tests that detect adenomas and polyps can actually prevent the development of cancer because these tests allow growths that might otherwise become cancer to be detected and removed. That is, colorectal cancer screening may be a form of cancer prevention, not just early detection.
Stool DNA test
A new type of non-invasive test to check for colon cancer and rectal cancer is available now, and may appeal to people who want to be screened, but don’t want to undergo the usual preparation required for a colonoscopy and some other screening tests. It’s called a stool DNA test because it looks for certain gene changes that are sometimes found in colon cancer and rectal cancer cells.
The FDA approved a stool DNA test called Cologuard in 2014. The patient uses a kit at home to collect a stool sample and mail it to a lab. The test checks for DNA changes that could be a sign of cancer or pre-cancerous growths called polyps. It also checks for blood in the stool, which can be a sign of cancer.
No special diet or bowel preparation (no laxatives or enemas) are required for a stool DNA test. However, if the Cologuard test does show a possible cancer or pre-cancer, the patient would then need a colonoscopy to confirm it, and possibly to remove any polyps.
Not everybody can have this type of screening test. It’s only for people with an average risk for colon or rectal cancer: no personal history of pre-cancerous polyps, colon or rectal cancer, or some other colon problems. Ask your doctor to be sure.
Tried-and-true screening tests
There are several more common tests that can be used to screen for colon and rectal cancer. Some are less able to find polyps and more likely to find cancer. Other tests not only can find cancer, but also are better at finding polyps; these tests may be more likely to prevent colon or rectal cancer.
Tests that can find polyps and cancer:
-
Colonoscopy
Colonoscopy uses a flexible lighted tube with a small camera on the end to look at the entire length of the colon and rectum. If polyps are found, they may be removed during the test. To prepare for the test, you may be asked to follow a special diet for a day or two before the test. You will also need to clean out your colon with strong laxatives (called a bowel prep) and sometimes with enemas, as well. Most people are sedated during the test. If nothing is found during the test, you won’t need another one for 10 years.
-
Flexible sigmoidoscopy
Flexible sigmoidoscopy is much like colonoscopy, but looks at only part of the colon and rectum. If polyps are found, they may be removed during the test, or you may need to have a colonoscopy later. Bowel prep may be required, but is not as extensive as the one used for colonoscopy. Most people do not need to be sedated during this test. If polyps or suspicious areas are seen, a colonoscopy will be needed to look at the rest of the colon. Flexible sigmoidoscopy must be done every 5 years.
-
Double-contrast barium enema
Double-contrast barium enema is a type of x-ray test. It involves putting a liquid called barium into the rectum, which spreads through the colon. Air is then pumped in to spread the barium in a thin, smooth layer to show better detail. Then x-rays are taken. It requires bowel prep, but no sedation. If polyps or suspicious areas are seen on the test, a follow-up colonoscopy will be needed. Barium enemas also need to be repeated every 5 years.
-
CT colonography
CT colonography (also called virtual colonoscopy) is a scan of the colon and rectum that produces detailed cross-sectional images so the doctor can look for polyps or cancer. It requires bowel prep, but no sedation. Air is pumped into the rectum and colon, and then a CT scanner is used to take images of the colon. If something is seen that may need to be biopsied, a follow-up colonoscopy will be needed. CT colonography must be done every 5 years.
Tests that mainly find cancer:
-
Guaiac-based fecal occult blood test (gFOBT) and fecal immunochemical test (FIT)
Guaiac-based fecal occult blood test (gFOBT) and fecal immunochemical test (FIT) are used to find tiny amounts of blood in the stool that could be a sign of cancer or large polyps. People take these tests at home with a kit they receive from their doctor’s office, along with instructions. A positive result will need to be followed up with a colonoscopy. However, many times the cause is a non-cancerous condition, such as ulcers or hemorrhoids. Stool tests like these need to be done every year.
Talk to your doctor about screening
Regular screening is one of the most powerful weapons for preventing colon cancer. If polyps are found during colon and rectal cancer testing, they can usually be removed before they have the chance to turn into cancer. Testing can also result in finding cancer early, when it’s smaller, easier to treat, and more likely to be curable.
If you’re 50 or older, talk to your doctor about which test is right for you and get tested as often as recommended. People at higher risk for colon or rectal cancer because of family history or certain health conditions (such as inflammatory bowel disease) may might need to start screening earlier.
What methods are used to screen people for colorectal cancer?
Expert medical groups, including the U.S. Preventive Services Task Force (USPSTF) strongly recommend screening for colorectal cancer. Although minor details of the recommendations may vary, these groups generally recommend that people at average risk of colorectal cancer get screened at regular intervals beginning at age 50 years.
The USPSTF recommends that screening continue to age 75 years; after age 75, the decision to screen is based on patient’s life expectancy, health status, comorbid conditions, and prior screening results. Routine screening of people aged 86 years or older is not recommended by the USPSTF.
People at increased risk because of a family history of colorectal cancer or polyps or because they have inflammatory bowel disease or certain inherited conditions may be advised to start screening before age 50 and/or have more frequent screening.
The USPSTF considers the following methods to be acceptable screening tests for colorectal cancer:
High-sensitivity fecal occult blood tests (FOBT).
Both polyps and colorectal cancers can bleed, and FOBT checks for tiny amounts of blood in feces (stool) that cannot be seen visually. (Blood in stool may also indicate the presence of conditions that are not cancer, such as hemorrhoids.)
Currently, two types of FOBT are approved by the Food and Drug Administration (FDA) to screen for colorectal cancer: guaiac FOBT (gFOBT) and the fecal immunochemical (or immunohistochemical) test (FIT, also known as iFoBT). With both types of FOBT, stool samples are collected by the patient using a kit, and the samples are returned to the doctor.
Guaiac FOBT uses a chemical to detect heme, a component of the blood protein hemoglobin. Because the guaiac FOBT can also detect heme in some foods (for example, red meat), people have to avoid certain foods before having this test.
FIT uses antibodies to detect human hemoglobin protein specifically. Dietary restrictions are typically not required for FIT.
Studies have shown that guaiac FOBT, when performed every 1 to 2 years in people aged 50 to 80 years, can help reduce the number of deaths due to colorectal cancer by 15 to 33%. If FOBT is the only type of colorectal cancer screening test performed, experts generally recommend yearly testing.
- Stool DNA test (FIT-DNA). The only stool DNA test approved by the FDA to date, Cologuard, is a multitarget test that detects tiny amounts of blood in stool (with an immunochemical test similar to FIT) as well as nine DNA biomarkers in three genes that have been found in colorectal cancer and precancerous advanced adenomas.
- The DNA comes from cells in the lining of the colon and rectum that are shed and collect in stool as it passes through the large intestine and rectum. As with both types of FOBT, the stool sample for the FIT-DNA test is collected by the patient using a kit; the sample is mailed to a laboratory for testing. A computer program analyzes the results of the two tests (blood and DNA biomarkers) and provides a finding of negative or positive. People who have a positive finding with this test are advised to have a colonoscopy.
In one study of people who were at average risk of developing colon cancer and had no symptoms of colon problems , this test detected more cancers and adenomas than the FIT test (that is, it was more sensitive). However, the FIT-DNA test also was more likely to identify an abnormality when none was actually present (that is, it had more false-positive results).
Sigmoidoscopy.
In this test, the rectum and sigmoid colon are examined using a sigmoidoscope, a flexible lighted tube with a lens for viewing and a tool for removing tissue. This instrument is inserted through the anus into the rectum and sigmoid colon as air (or carbon dioxide) is pumped into the colon to expand it so the doctor can see the colon lining more clearly. During sigmoidoscopy, abnormal growths in the rectum and sigmoid colon can be removed for analysis (biopsied). The lower colon must be cleared of stool before sigmoidoscopy, but the preparation is less extensive than that required for colonoscopy. People are usually not sedated for this test.
Studies have shown that people who have regular screening with sigmoidoscopy after age 50 years have a 60 to 70% lower risk of death due to cancer of the rectum and lower colon than people who do not have screening.One randomized controlled clinical trial found that even just one sigmoidoscopy screening between 55 and 64 years of age can substantially reduce colorectal cancer incidence and mortality .Experts generally recommend sigmoidoscopy every 5 years with or without gFOBT or FIT every 3 years for people at average risk who have had negative test results.
Standard (or optical) colonoscopy.
In this test, the rectum and entire colon are examined using a = colonoscope ,a flexible lighted tube with a lens for viewing and a tool for removing tissue. Like the shorter sigmoidoscope, the colonoscope is inserted through the anus into the rectum and the colon as air (or carbon dioxide) is pumped into the colon to expand it so the doctor can see the colon lining more clearly.
During colonoscopy, any abnormal growths in the colon and the rectum can be removed, including growths in the upper parts of the colon that are not reached by sigmoidoscopy. A thorough cleansing of the entire colon is necessary before this test. Most patients receive some form of sedation during the test.
Studies suggest that colonoscopy reduces deaths from colorectal cancer by about 60 to 70%. Additional studies are currently being done to better evaluate how effective colonoscopy screening methods are. Experts recommend colonoscopy every 10 years for people at average risk as long as their test results are negative.
Virtual colonoscopy.
This screening method, also called computed tomographic (CT) colonography, uses special x-ray equipment (a CT scanner) to produce a series of pictures of the colon and the rectum from outside the body. A computer then assembles these pictures into detailed images that can show polyps and other abnormalities. Virtual colonoscopy is less invasive than standard colonoscopy and does not require sedation.
As with standard colonoscopy, a thorough cleansing of the colon is necessary before this test, and air (or carbon dioxide) is pumped into the colon to expand it for better viewing of the colon’s lining. The accuracy of virtual colonoscopy is similar to that of standard colonoscopy, and virtual colonoscopy has a lower risk of complications. However, if polyps or other abnormal growths are found during a virtual colonoscopy, a standard colonoscopy is usually performed to remove them.
Whether virtual colonoscopy can help reduce deaths from colorectal cancer is not yet known, and Medicare and some insurance companies currently do not pay for the costs of this procedure. Studies are ongoing to compare virtual colonoscopy with other screening methods.
Several other tests to screen for colorectal cancer exist, although these are not generally recommended.
Double-contrast barium enema.
This test, also called DCBE, is another method of visualizing the colon from outside the body. In DCBE, a series of x-ray images of the entire colon and rectum is taken after the patient is given an enema with a barium solution. The barium helps to outline the colon and the rectum on the images. DCBE is rarely used for screening because it is less sensitive than colonoscopy in detecting small polyps and cancers. However, it may be used for people who cannot undergo standard colonoscopy for example, because they are at particular risk for complications.
Single-specimen guaiac FOBT done in a doctor’s office.
Doctors sometimes perform a single-specimen guaiac FOBT on a stool sample collected during a digital rectal examination as part of a routine physical examination. However, this approach has not been shown to be an effective way to screen for colorectal cancer.
Screening is so important because early colorectal cancer usually has no symptoms. If there are symptoms, here’s what you should look out for:
- Bleeding from the rectum or blood in the stool
- Abdominal discomfort, such as cramps, gas or pain, that persists
- Change in bowel habits, including diarrhea, constipation or a change in consistency of your stool
- Feeling that your bowel doesn’t empty completely
- Losing weight for no apparent reason
- Loss of appetite
- Fatigue
- Dark or black stools
In addition to screening, you can do these things to lower your risk:
-
Exercise.
A recent review of scientific literature found that the most physically active people have a 25 percent lower risk of colon cancer than the least active people. The American Cancer Society and the CDC recommend at least 150 minutes a week of moderate-intensity activity or 75 minutes of vigorous activity each week.
-
Maintain a healthy weight.
Being overweight or obese increases your risk for colon cancer; this is especially true for men. The most important risk factor is having that extra weight around your waist. Abdominal obesity is a more important risk factor than is overall obesity.
-
Eat a healthy diet.
Research is ongoing, but what is known is that a high consumption of red and/or processed meats put you at increased risk. To reduce your risk, increase your intake of dietary fiber, cereal fiber and whole grains. Moderate intake of fruits and veggies can be protective, too. Eat at least 2 1/2 cups each day.
-
Get your dairy.
There is a protective effect (regardless of milk fat content) with a higher consumption of dairy product, milk and calcium.
-
Limit alcohol.
It’s estimated that people who average between two and four alcoholic drinks a day throughout their lifetime have a 23 percent higher risk of colorectal cancer than those who consume less than one drink a day.
-
Quit smoking.
Enough said.
When you’re ready to discuss screening with your health care provider (and I’m hoping you are), there are many options to explore. Besides a standard (or optical) colonoscopy, there’s high-sensitivity fecal occult blood tests, sigmoidoscopy, virtual colonoscopy, double-contrast barium enema and Colorguard, a new test that was approved by the FDA in 2014.
For more information visit us our website: https://www.healthinfi.com
0 200


No Comments