Treatment for Brain and Spinal Cord Tumors in Children
Children with brain or spinal cord tumors require special care because their brains and bodies are still developing. The treatment will depend on many factors, including:
- The location of the brain or spinal cord tumor
- Whether it is benign or malignant
- The child’s age and general health
- The parents’ preferences regarding treatment options
- The risks associated with a particular treatment
Surgery is the most common treatment for children with brain and spinal cord tumors. If the child’s tumor is benign and in a part of the brain where neurosurgeons can safely completely remove it, surgery is likely to be the only treatment needed.
Doctors commonly use radiation therapy after surgery for tumors that neurosurgeons cannot completely remove and for the most malignant tumors. Radiation therapy may also used to treat tumors in locations where surgery is not safe. However, radiation therapy is not used in very young children because it may affect the developing brain.
If the tumor is malignant and growing rapidly, doctors may recommend chemotherapy.
For a small brain or spinal cord tumor that does not cause any significant signs or symptoms, monitoring the tumor without any immediate treatment, called observation, may be an option. If the tumor does not grow, the child may not need treatment.
Cerebrum and spinal string tumors are masses of strange cells in the mind or spinal string that have become wild. Cells in almost any piece of the body can move toward becoming disease, and can spread to different territories of the body. To take in more about how tumors begin and spread.
In most different parts of the body, it is essential to recognize favorable (non-dangerous) and threatening (carcinogenic) tumors. Generous tumors don’t attack close-by tissues or spread to inaccessible regions, so in different parts of the body they are never perilous. One of the primary reasons threatening tumors (malignancies) are so hazardous is on the grounds that they can spread all through the body.
In spite of the fact that mind tumors once in a while spread to different parts of the body, a large portion of them can spread through the cerebrum and spinal line tissue. Indeed, even supposed benevolent tumors can, as they develop, press on and devastate ordinary mind tissue, causing harm that is regularly impairing and can in some cases cause demise. This is the reason specialists ordinarily talk about “cerebrum tumors” as opposed to “mind malignancies.” The fundamental worries with cerebrum and spinal string tumors are the means by which quick they develop, how promptly they spread through whatever is left of the cerebrum or spinal line, and in the event that they can be evacuated or treated and not return. In any case, both benevolent and harmful tumors can be perilous.
Cerebrum and spinal rope tumors in kids have a tendency to be not the same as those in grown-ups. They regularly frame in better places, create from various cell composes, and may have an alternate treatment and visualization (viewpoint). For data about the contrasts between youth malignancies and grown-up diseases, see Tumor in Kids.
The focal sensory system
To comprehend mind and spinal string tumors, it thinks about the ordinary structure and capacity of the focal sensory system (CNS), which is the therapeutic name for the cerebrum and spinal rope.
The mind is the focal point of thought, feeling, memory, discourse, vision, hearing, development, and substantially more. The spinal line and unique nerves in the head called cranial nerves convey messages between the cerebrum and whatever is left of the body. These messages advise our muscles how to move, transmit data accumulated by our faculties, and help facilitate the elements of our inward organs.
The cerebrum is ensured by the skull. In like manner, the spinal rope is ensured by the bones (vertebrae) of the spinal segment.
The mind and spinal line are encompassed and padded by a fluid called cerebrospinal liquid (CSF). Cerebrospinal liquid is made by the choroid plexus, which is situated in spaces in the cerebrum called ventricles. The ventricles and the spaces around the mind and spinal rope are loaded with CSF.
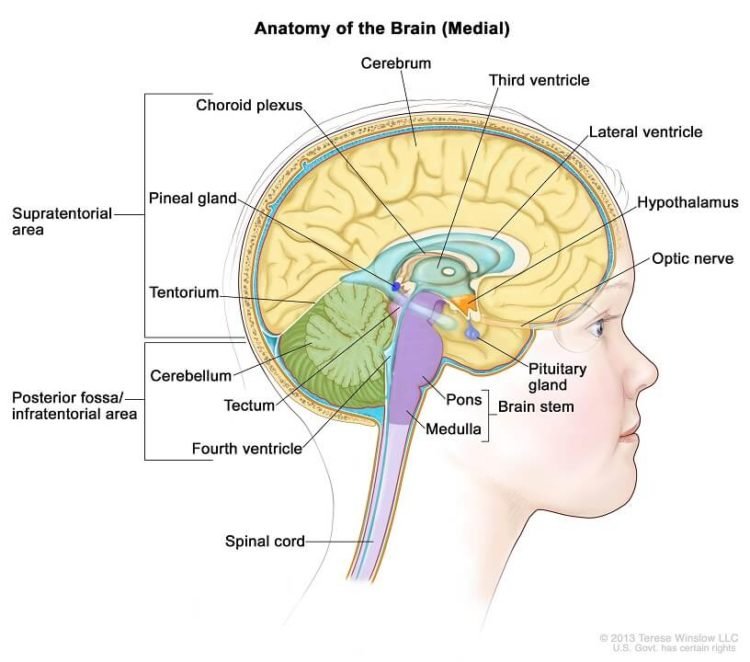
Parts of the mind and spinal line
outline demonstrating parts of the mind and spinal string including cerebrum, horizontal ventricle, pineal organ, third ventricle, cerebellum, fourth ventricle, cerebrum stem, spinal line, hypothalamus and pituitary (there is likewise a nearby cross segment demonstrating the skull, meninges, cerebrum)
The primary zones of the mind incorporate the cerebrum, cerebellum, and mind stem. Every territory has an uncommon capacity.
Cerebrum: The cerebrum is the extensive, external piece of the mind. It is comprised of 2 sides of the equator (parts) and controls thinking, thought, feeling, and dialect. It is likewise in charge of arranged (willful) muscle developments (tossing a ball, strolling, biting, and so on.) and for taking in and translating tangible data, for example, vision, hearing, notice, touch, and agony.
The side effects caused by a tumor in a cerebral side of the equator rely upon where the tumor is. Regular side effects include:
Seizures
Inconvenience talking
A difference in state of mind, for example, dejection
An adjustment in identity
Shortcoming or loss of motion in part of the body
Changes in vision, hearing, or different faculties
Cerebellum: The cerebellum lies under the cerebrum at the back piece of the mind. It helps arrange development.
Tumors of the cerebellum can cause issues with coordination in strolling; issue with exact developments of hands, arms, feet, and legs; issues with gulping or synchronized eye developments; and changes in discourse mood. Mind stem: The cerebrum stem is the lower some portion of the mind that associates with the spinal line. It has groups of long nerve strands that convey signals controlling muscles and sensation or feeling between the cerebrum and whatever is left of the body. Exceptional focuses in the cerebrum stem additionally help control breathing and the heart pulsating. Moreover, most cranial nerves (depicted underneath) begin in the mind stem.
The cerebrum stem is separated into 3 primary parts: the midbrain, pons, and medulla oblongata.
Tumors in this basic zone of the mind can cause shortcoming, solid muscles, or issues with sensation, facial or eye development, hearing, or gulping. Twofold vision is a typical early side effect of mind stem tumors, as are issues with coordination in strolling. Since the cerebrum stem is a little zone that is so fundamental forever, it won’t not be conceivable to surgically expel tumors around there.
Spinal string: The spinal line has groups of long nerve strands that convey signals that control muscles, sensation or feeling, and bladder and entrail control.
Spinal rope tumors can cause shortcoming, loss of motion, or deadness. The spinal rope is a thin structure, so tumors that create there as a rule cause manifestations on the two sides of the body (for instance, shortcoming or deadness of the two legs). This is not quite the same as indications of most mind tumors, which frequently influence just a single side of the body. The nerves that achieve the arms leave the spinal line at the level of the neck (cervical spine). Nerves to the legs, gut, and bladder fan out the spinal line in the back (thoracic and lumbar spine). Spinal string tumors in the neck (cervical spine) can cause manifestations in both the arms and legs, and also influence gut and bladder work. Spinal rope tumors underneath the neck just influence the legs and inside and bladder work.
representation demonstrating the area of the cranial nerves, spinal nerves, fringe nerves and focal sensory system (cerebrum, cerebellum, spinal line)
Cranial nerves: The cranial nerves broaden specifically out of the base of the cerebrum (rather than leaving the spinal rope). These nerves convey flags specifically between the mind and the face, eyes, tongue, mouth, and some different territories. The most widely recognized cranial nerve tumors in youngsters are called optic gliomas, which are tumors of the optic nerve (the expansive nerve that keeps running between the mind and each eye). These tumors cause vision issues. Tumors beginning in other cranial nerves can cause twofold vision; inconvenience gulping; hearing misfortune in one or the two ears; or facial loss of motion, deadness, or agony.
Types of cells and body tissues in the brain and spinal cord
The brain and spinal cord have many kinds of tissues and cells, which can develop into different types of tumors. Neurons (nerve cells): These are the most important cells in the brain. They transmit chemical and electric signals that determine thought, memory, emotion, speech, muscle movement, sensation, and just about everything else that the brain and spinal cord do. Neurons send these signals through their nerve fibers (axons). Axons in the brain tend to be short, while those in the spinal cord can be as long as several feet. Unlike many other types of cells that can grow and divide to repair damage from injury or disease, neurons in the brain and spinal cord largely stop dividing about a year after birth (with a few exceptions). Neurons do not usually form tumors, but they can be damaged by tumors that start nearby.
Glial cells: Glial cells are the supporting cells of the brain. Most brain and spinal cord tumors develop from glial cells. These tumors are sometimes referred to as a group called gliomas. There are 3 types of glial cells – astrocytes, oligodendrocytes, and ependymal cells. A fourth cell type called microglia is part of the immune system and is not truly a glial cell.
Astrocytes help support and nourish neurons. When the brain is injured, astrocytes form scar tissue that helps repair the damage. The main tumors starting in these cells are called astrocytomas or glioblastomas. Oligodendrocytes make myelin, a fatty substance that surrounds and insulates the nerve cell axons of the brain and spinal cord. This helps neurons send electric signals through the axons. Tumors starting in these cells are called oligodendrogliomas.
Ependymal cells line the ventricles (fluid-filled areas) within the central part of the brain and form part of the pathway through which cerebrospinal fluid (CSF) flows. Tumors starting in these cells are called ependymomas.
Microglia are the immune (infection fighting) cells of the central nervous system.
Neuroectodermal cells: These are very early forms of nervous system cells that are probably involved in brain cell development. They are found throughout the brain. The most common tumors that come from these cells are called medulloblastomas, which start in the cerebellum. Meninges: These are layers of tissue that line and protect the brain and spinal cord. The meninges help form the spaces through which CSF travels. The most common tumors that start in these tissues are called meningiomas.
Choroid plexus: The choroid plexus is the area of the brain within the ventricles that makes CSF, which nourishes and protects the brain. Tumors that start here include choroid plexus papillomas and choroid plexus carcinomas.
Pituitary gland and hypothalamus: The pituitary is a small gland at the base of the brain. It is connected to a part of the brain called the hypothalamus. Both make hormones that help regulate the activity of several other glands in the body. For example, they control the amount of thyroid hormone made by the thyroid gland, the production and release of milk by the breasts, and the amount of male or female hormones made by the testicles or ovaries. They also make growth hormone, which stimulates body growth, and vasopressin, which regulates water balance by the kidneys.
The growth of tumors in or near the pituitary or hypothalamus, as well as surgery and/or radiation therapy in this area, can affect these functions. For example, tumors starting in the pituitary gland sometimes make too much of a certain hormone, which can cause problems. On the other hand, a child may have low levels of one or more hormones after treatment and may need to take hormones to make up for this. Pineal gland: The pineal gland is not really part of the brain. It is a small endocrine gland that sits between the cerebral hemispheres. It makes melatonin, a hormone that regulates sleep, in response to changes in light. The most common tumors of the pineal gland are called pineoblastomas.
Blood-brain barrier: The inner lining of the small blood vessels (capillaries) in the brain and spinal cord creates a very selective barrier between the blood and the tissues of the central nervous system. This barrier normally helps maintain the brain’s metabolic balance and keeps harmful toxins from getting into the brain. Unfortunately, it also keeps out most chemotherapy drugs that are used to kill cancer cells, which in some cases limits their usefulness.
Types of Brain and Spinal Cord Tumors in Children
Tumors can form in almost any type of tissue or cell in the brain or spinal cord. Some tumors have a mixture of cell types. Tumors in different areas of the central nervous system may be treated differently and have a different prognosis (outlook).
Brain tumors in children are more likely to start in the lower parts of the brain, such as the cerebellum and brain stem, than they are in adults. But they can start in the upper parts of the brain as well.
Gliomas
Gliomas are not a specific type of tumor. Glioma is a general term for a group of tumors that start in glial cells. A number of tumors can be considered gliomas, including glioblastoma (also known as glioblastoma multiforme), anaplastic astrocytoma, astrocytoma, oligodendroglioma, ependymoma, brain stem glioma, and optic glioma. About half of all brain and spinal cord tumors in children are gliomas.
Astrocytomas
Astrocytomas are tumors that start in cells called astrocytes, a kind of glial cell.
Most astrocytomas can spread widely throughout the brain and blend with the normal brain tissue, which can make them very hard to remove by surgery. Sometimes they spread along the cerebrospinal fluid (CSF) pathways. It is very rare for them to spread outside of the brain or spinal cord.
Astrocytomas are often grouped as high grade, intermediate grade, or low grade, based largely on how the cells look under the microscope.
Intermediate- and high-grade astrocytomas: These tumors tend to grow quickly and spread into the surrounding normal brain tissue. The highest-grade astrocytoma, known as glioblastoma, is the fastest growing. Anaplastic astrocytomas are also in this group. Low-grade astrocytomas: These tumors tend to grow slowly and are the most common type in children. Some special types, known as non-infiltrating astrocytomas, tend to grow very slowly and do not grow into (infiltrate) nearby tissues, so they often have a good prognosis.
Pilocytic astrocytomas are slow growing and rarely infiltrate nearby tissues. They most commonly occur in the cerebellum but can also begin in the optic nerve, hypothalamus, brain stem, or other areas. They account for nearly 1 out of 5 brain tumors in children.
Subependymal giant cell astrocytomas (SEGAs) occur in the ventricles. They are also slow growing and rarely infiltrate nearby tissues. These tumors are almost always linked with an inherited condition called tuberous sclerosis. Fibrillary (diffuse) astrocytomas are also slow-growing tumors, but with the important characteristic of growing into nearby tissues, which makes them hard to remove with surgery. Though these tumors are thought of as low grade, they tend to become more aggressive and fast growing over time.
Optic gliomas are low-grade astrocytomas that start in the optic nerves (the nerves leading from the eyes to the brain). They are often linked with an inherited condition called neurofibromatosis type 1. These tumors are rarely fatal, but they may cause vision loss and injury to nearby brain tissue.
Oligodendrogliomas
These tumors start in brain glial cells called oligodendrocytes. These tumors tend to grow slowly, but like astrocytomas, most of them can grow into nearby brain tissue and can’t be removed completely by surgery. Oligodendrogliomas rarely spread along the CSF pathways and even less frequently spread outside the brain or spinal cord. Only about 1% of brain tumors in children are oligodendrogliomas. As with astrocytomas, they can become more aggressive over time.
Ependymomas
About 5% of brain tumors in children are ependymomas. These tumors start in the ependymal cells that line the ventricles or central canal of the spinal cord. They can range from fairly low-grade (slow growing) tumors to higher grade ones, which are called anaplastic ependymomas.
Ependymomas may spread along the CSF pathways but do not spread outside the brain or spinal cord. These tumors can block the flow of CSF out of the ventricles, causing the ventricles to become very large – a condition called hydrocephalus.
Unlike astrocytomas and oligodendrogliomas, ependymomas usually do not grow into normal brain tissue. As a result, some (but not all) ependymomas can be removed and cured by surgery. But because they can spread along ependymal surfaces and CSF pathways, treating them can sometimes be difficult.
Mixed gliomas
These tumors contain more than one cell type. For example, oligoastrocytomas have some of the same types of cells as both oligodendrogliomas and astrocytomas. Treatment is typically based on the fastest-growing component of the tumor.
Brain stem gliomas
This term refers to the location of the tumor, rather than the type of cell it starts in. A small number of brain stem gliomas occur as a tumor with very distinct edges (called a focal brain stem glioma). More often, brain stem gliomas grow diffusely throughout the brain stem, rather than growing as a focal tumor. These tumors often start in the pons, where they are called diffuse intrinsic pontine gliomas (DIPGs).
About 10% to 20% of brain tumors in children are brain stem gliomas. Nearly all of these tumors are some type of astrocytoma.
Primitive neuroectodermal tumors (PNETs)
These tumors start in primitive (immature) cells of the central nervous system called neuroectodermal cells. About 1 out of 5 brain tumors in children are PNETs. They are more common in younger children than older ones, and are rare in adults. PNETs tend to grow quickly and often spread throughout the CSF pathways.
Medulloblastomas: PNETs that start in the cerebellum are called medulloblastomas. Most PNETs in children are medulloblastomas. These tumors can often be treated effectively and tend to have a better outlook than PNETs in other parts of the brain. Pineoblastomas: PNETs that occur in the pineal gland are called pineoblastomas. These tumors are usually harder to treat than medulloblastomas. Other PNETs: Other, less common types of central nervous system PNETs include medulloepitheliomas, ependymoblastomas, and neuroblastomas that start in the brain or spinal cord.
Craniopharyngiomas
These slow-growing tumors start above the pituitary gland but below the brain itself. They account for about 4% of brain tumors in children. These tumors may press on the pituitary gland and the hypothalamus, causing hormone problems. Because craniopharyngiomas start very close to the optic nerves, they can also cause vision problems. This makes them hard to remove completely without damaging the child’s vision or hormone balance.
Mixed glial and neuronal tumors
Certain tumors that develop in children and young adults (and rarely in older adults) have both glial and neuronal cell components. They tend to have a fairly good prognosis.
Pleomorphic xanthoastrocytoma (PXA) and dysembryoplastic neuroepithelial tumors (DNETs) look as if they could grow quickly when seen under the microscope, but these tumors tend to be fairly benign, and most are cured by surgery alone.
Ganglioglioma is a type of tumor that has both mature neurons and glial cells. Most can be cured by surgery alone or surgery combined with radiation therapy.
Choroid plexus tumors
These rare tumors start in the choroid plexus within the ventricles of the brain. Most are benign (choroid plexus papillomas) and are cured by surgery. However, some are malignant (choroid plexus carcinomas).
Schwannomas (neurilemmomas)
This type of tumor starts in Schwann cells that surround and insulate cranial nerves and other nerves. Schwannomas are usually benign tumors. They often form near the cerebellum on the cranial nerve responsible for hearing and balance, in which case they are called vestibular schwannomas or acoustic neuromas. They may also develop on spinal nerves past the point where the nerves have left the spinal cord. When this is the case, the tumor can press on the spinal cord, causing weakness, sensory loss, and bowel and bladder problems.
These tumors are rare in children. When schwannomas are found in a child, particularly if there are tumors on both sides of the head, it often means the child has an inherited tumor syndrome such as neurofibromatosis type 2 (see What are the risk factors for brain and spinal cord tumors in children?).
Other tumors that start in or near the brain
Meningiomas
These tumors begin in the meninges, the layers of tissue that surround the outer part of the brain and spinal cord. Meningiomas cause symptoms by pressing on the brain or spinal cord. They are much less common in children than in adults.
Meningiomas are almost always benign and are usually cured by surgery. Some, however, are located very close to vital structures in the brain and can’t be cured by surgery alone.
Meningiomas are often assigned a grade based on how the tumor cells look.
Grade I tumors, which look most like normal cells, make up about 80% to 90% of meningiomas.
Grade II (atypical) meningiomas look slightly more abnormal.
Grade III (anaplastic) meningiomas, which look the most abnormal, make up only about 1% to 3% of meningiomas.
Higher-grade meningiomas are more likely to come back after treatment, and some grade III meningiomas can spread to other parts of the body.
Chordomas
These tumors start in the bone at the base of the skull or at the lower end of the spine. These tumors don’t start in the central nervous system, but they can injure nearby parts of the brain or spinal cord by pressing on them. Chordomas tend to come back after treatment, if they are not removed completely, causing more damage. They usually do not spread to other organs. Chordomas are much more common in adults than in children. For more on these tumors, see Bone Cancer.
Germ cell tumors
These rare tumors develop from germ cells, which normally form eggs in women and sperm in men. During normal development before birth, germ cells travel to the ovaries or testicles and develop into eggs or sperm cells. But sometimes some germ cells don’t move where they should and end up in abnormal locations such as the brain. They may then develop into germ cell tumors, similar to those that can form in the ovaries or testicles.
Germ cell tumors of the nervous system usually occur in children, most often in the pineal gland or above the pituitary gland. These tumors can sometimes be diagnosed without a biopsy by measuring certain chemicals in the cerebrospinal fluid (CSF) or blood.
The most common germ cell tumor of the nervous system is the germinoma. Other tumors that start in germ cells include choriocarcinomas, embryonal carcinomas, teratomas, and yolk sac tumors (endodermal sinus tumors).
Neuroblastomas
These nerve cell tumors are the third most common cancer in children. Neuroblastomas rarely develop in the brain or spinal cord; most develop from nerve cells inside the abdomen or chest. This type of cancer is most common during early infancy. For more information, see Neuroblastoma.
Lymphomas
Lymphomas are cancers that start in cells called lymphocytes (one of the main cell types of the immune system). Most lymphomas start in other parts of the body, but a small portion start in the central nervous system (CNS). CNS lymphomas are rare in children. For more on childhood lymphomas, see Non-Hodgkin Lymphoma in Children.
Pituitary tumors
Tumors that start in the pituitary gland are almost always benign (non-cancerous). But they can still cause problems if they grow large enough to press on nearby structures or if they make too much of any kind of hormone. These tumors are more common in teens than in younger children. For more information, see our document Pituitary Tumors.
Cancers that spread to the brain from other sites
Sometimes brain tumors are found not to have started in the brain but rather to have metastasized (spread) there from some other part of the body. Tumors that start in other organs and then spread to the brain are called metastatic or secondary brain tumors (as opposed to primary brain tumors, which start in the brain). This is important because metastatic and primary brain tumors are often treated differently. In children, metastatic brain tumors are much less common than primary brain tumors. Childhood leukemias can sometimes spread to the CSF around the brain and spinal cord. When this happens, the cancer is still considered a leukemia (the cancer cells in the CSF are leukemia cells), so doctors use treatments directed at the leukemia. For more information, see Childhood Leukemia.
Risk Factors
A risk factor is anything that affects a person’s chance of getting a disease such as a brain or spinal cord tumor. Different types of cancer have different risk factors. Lifestyle-related risk factors such as diet, body weight, physical activity, and tobacco use play a major role in many adult cancers. But these factors usually take many years to influence cancer risk, and they are not thought to play much of a role in childhood cancers, including brain tumors. Very few risk factors have been found for brain and spinal cord tumors. There is no clear cause for most of these tumors.
Radiation exposure
The only well-established environmental risk factor for brain tumors is radiation exposure to the head, which most often comes from the treatment of other conditions. For example, before the risks of radiation were well known (more than 50 years ago), children with ringworm of the scalp (a fungal infection) often received low-dose radiation therapy. This was later found to increase their risk of brain tumors as they got older.
Today, most radiation-induced brain tumors are caused by radiation given to the head to treat other cancers, such as leukemia. These brain tumors usually develop around 10 to 15 years after the radiation.
Radiation-induced tumors are still fairly rare, but because of the increased risk (as well as the other side effects), radiation therapy is only given to the head after carefully weighing the possible benefits and risks. For most patients with cancer in or near the brain, the benefits of getting radiation therapy as part of their treatment far outweigh the small risk of developing a brain tumor years later.
The possible risk from fetal or childhood exposure to imaging tests that use radiation, such as x-rays or CT scans, is not known for sure. These tests use much lower levels of radiation than those used in radiation treatments, so if there is any increase in risk, it is likely to be very small. But to be safe, most doctors recommend that pregnant women and children not get these tests unless they are absolutely needed.
Inherited and genetic conditions
In rare cases (less than 5% of brain tumors), children have inherited abnormal genes from a parent that put them at increased risk for certain types of brain tumors. In other cases, these abnormal genes are not inherited but occur as a result of changes (mutations) in the gene before birth.
People with inherited tumor syndromes often have many tumors that start when they are young. Some of the more well-known syndromes include:
Neurofibromatosis type 1 (von Recklinghausen disease)
This is the most common syndrome linked to brain or spinal cord tumors. It is often inherited from a parent, but it can also start in some children whose parents don’t have it. Children with this syndrome may have optic gliomas or other gliomas of the brain or spinal cord, or neurofibromas (benign tumors of peripheral nerves). Changes in the NF1 gene cause this disorder.
Neurofibromatosis type 2
Less common than von Recklinghausen disease, this condition can also either be inherited or may start in children without a family history. It is associated with cranial or spinal nerve schwannomas, especially vestibular schwannomas (acoustic neuromas), which almost always occur on both sides of the head. It is also linked to an increased risk of meningiomas, as well as spinal cord gliomas or ependymomas. Changes in the NF2 gene are responsible for neurofibromatosis type 2.
Tuberous sclerosis
Children with this condition may develop subependymal giant cell astrocytomas (SEGAs), as well as other benign tumors of the brain, skin, heart, kidneys, or other organs. This condition is caused by changes in either the TSC1 or the TSC2 gene.
Von Hippel-Lindau disease
Children with this disease tend to develop blood vessel tumors (hemangioblastomas) of the cerebellum, spinal cord, or retina, as well as tumors in the kidney, pancreas, and some other parts of the body. It is caused by changes in the VHL gene.
Li-Fraumeni syndrome
People with this syndrome have an increased risk of gliomas, as well as breast cancer, soft tissue sarcomas, leukemia, adrenal gland cancer, and some other types of cancer. It is caused by changes in the TP53 gene.
Other syndromes
Other inherited conditions linked with increased risks of certain types of brain and spinal cord tumors include:
Gorlin syndrome (basal cell nevus syndrome)
Turcot syndrome
Cowden syndrome
Hereditary retinoblastoma
Rubinstein-Taybi syndrome
Some families may have genetic disorders that are not well recognized or that could even be unique to a particular family.
Factors with uncertain, controversial, or unproven effects on brain tumor risk
Cell phone use
Cell phones give off radiofrequency (RF) rays, a form of electromagnetic energy on the spectrum between FM radio waves and those used in microwave ovens, radar, and satellite stations. Cell phones do not give off ionizing radiation, the type that can cause cancer by damaging the DNA inside cells. Still, there have been concerns that the phones, whose antennae are built-in and therefore are placed close to the head when being used, might somehow raise the risk of brain tumors.
Some studies have suggested a possible increased risk of brain tumors or of vestibular schwannomas in adults with cell phone use, but most of the larger studies done so far have not found an increased risk, either overall or among specific types of tumors. Still, there are very few studies of long-term use (10 years or more), and cell phones haven’t been around long enough to determine the possible risks of lifetime use. The same is true of any possible higher risks in children, who are increasingly using cell phones. Cell phone technology also continues to change, and it’s not clear how this might affect any risk.
These risks are being studied, but it will likely be many years before firm conclusions can be made. In the meantime, for people concerned about the possible risks, there are ways to lower their (and their children’s) exposure, such as using the speaker function or an earpiece to move the phone itself away from the head when used. For more information, see our document Cellular Phones.
Other factors
Exposure to aspartame (a sugar substitute), exposure to electromagnetic fields from power lines and transformers, and infection with certain viruses have been suggested as possible risk factors, but most researchers agree that there is no convincing evidence to link these factors to brain tumors. Research on these and other potential risk factors continues.
Causes
The cause of most brain and spinal cord tumors is not fully understood. But researchers have found some of the changes that occur in normal brain cells that may lead them to form tumors.
Normal human cells grow and function based mainly on the information contained in each cell’s chromosomes. Chromosomes are long strands of DNA in each cell. Brain and spinal cord tumors, like other tumors, are usually caused by changes (mutations) in the DNA inside cells. DNA is the chemical that makes up our genes – the instructions for how our cells function. We usually look like our parents because they are the source of our DNA. But DNA affects more than how we look.
Some genes control when our cells grow, divide into new cells, and die. Certain genes that help cells grow, divide, and stay alive are called oncogenes. Others that slow down cell division, or cause cells to die at the right time, are called tumor suppressor genes. Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes. These gene changes can be inherited from a parent (as is sometimes the case with childhood cancers), but more often they happen spontaneously during a person’s lifetime.
In recent years, researchers have found the gene changes that cause some rare inherited syndromes (like neurofibromatosis, tuberous sclerosis, Li-Fraumeni syndrome, and von Hippel-Lindau syndrome) and increase the risk of developing some brain and spinal cord tumors. For example, the Li-Fraumeni syndrome is caused by changes in the TP53 tumor suppressor gene. Normally, this gene prevents cells with damaged DNA from growing. Changes in this gene increase the risk of developing brain tumors (particularly gliomas), as well as some other cancers.
In most cases, it is not known why people without inherited syndromes develop brain or spinal cord tumors. Most risk factors for cancer somehow damage genes. For example, tobacco smoke is a risk factor for lung cancer and several other cancers because it contains chemicals that can damage genes. The brain is relatively protected from tobacco smoke and other cancer-causing chemicals that we might breathe in or eat, so these factors are not likely to play a major role in these cancers.
Several different gene changes must usually occur in normal cells before they become cancerous. There are many kinds of brain tumors, each of which may have different sets of gene changes. A number of gene or chromosome changes have been found in different brain tumor types, but there are probably many others that have not yet been found.
Researchers now understand some of the gene changes that occur in different types of brain tumors, but it’s still not clear what causes these changes. Some gene changes might be inherited, but most brain and spinal cord tumors in children are not the result of known inherited syndromes. Most gene changes are probably just random events that sometimes happen inside a cell, without having an outside cause.
Other than radiation, there are no known lifestyle-related or environmental causes of childhood brain tumors, so it is important to remember that there is nothing these children or their parents could have done to prevent these cancers.
Can Brain and Spinal Cord Tumors in Children Be Found Early?
Screening is testing for a disease (such as brain or spinal cord tumors) in people without any symptoms. At this time there are no widely recommended screening tests for most children to look for brain or spinal cord tumors before they start to cause symptoms. These tumors usually are found as a result of signs or symptoms the child is having.
Most often, the outlook for people with brain or spinal cord tumors depends on the type of tumor and its location, not how early it is detected. But as with any disease, earlier detection and treatment is likely to be helpful. For children with certain inherited syndromes that put them at higher risk for brain tumors, such as neurofibromatosis or tuberous sclerosis, doctors often recommend frequent physical exams and other tests. These tests might find tumors when they are still small. Not all tumors related to these syndromes may need to be treated right away, but finding them early might help doctors monitor them so that they can be treated quickly if they begin to grow or cause problems.
Signs and Symptoms
Signs and symptoms from brain and spinal cord tumors might occur gradually and become worse over time, or they can happen suddenly, such as with a seizure.
General symptoms
Tumors in any part of the brain might raise the pressure inside the skull (known as intracranial pressure). This can be caused by growth of the tumor, swelling in the brain, or blocked flow of cerebrospinal fluid. Increased pressure can lead to general symptoms such as:
Headache
Nausea
Vomiting
Crossed eyes or blurred vision
Balance problems
Behavior changes
Seizures
Drowsiness or even coma
Headaches that get worse over time are a common symptom of brain tumors. But not all brain tumors cause headaches, and most headaches are not caused by tumors.
In some children, seizures are the first symptom of a brain tumor. Most seizures in children are not caused by brain tumors, but if your child has a seizure, your child’s doctor may refer you to a neurologist (a doctor who specializes in brain and nervous system problems) to make sure it wasn’t caused by a brain tumor or other serious disease.
In the first few years of life, other symptoms of tumors can include irritability, loss of appetite, developmental delay, and a drop in intellectual and physical abilities. In very young children who can’t complain of symptoms, a parent may notice an increase in head size, sometimes along with bulging of the soft spots of the skull (fontanelles). This happens because the bones of the skull haven’t grown together yet, and increased pressure from a tumor can push them apart.
In the school-aged child, other general symptoms of tumors can include poor school performance, fatigue, and personality changes.
If the child can cooperate, the doctor can sometimes tell if pressure inside the skull is increased by looking inside the child’s eyes for swelling of the optic nerve (known as papilledema).
Symptoms of tumors in different parts of the central nervous system
Tumors in different parts of the brain or spinal cord can cause different symptoms. But these symptoms can be caused by any disease in that particular location – they don’t always mean a child has a brain or spinal cord tumor.
Brain and spinal cord tumors often cause problems with the specific functions of the region they develop in. For example:
Tumors in the parts of the cerebrum (the large, outer part of the brain) that control movement or sensation can cause weakness or numbness in a part of the body, often on just one side.
Tumors in or near the parts of the cerebrum responsible for language can cause problems with speech or even understanding words.
Tumors in the front part of the cerebrum can sometimes affect thinking, personality, and language skills.
Tumors in an area of the brain called the basal ganglia typically cause abnormal movements and body positions.
Tumors in the cerebellum, which controls coordination, can cause trouble walking or with other normal functions, even eating.
Tumors in the back part of the cerebrum, or around the pituitary gland, the optic nerves, or certain other cranial nerves can cause vision problems.
Tumors in or near other cranial nerves might lead to loss of hearing, balance problems, weakness of some facial muscles, or trouble swallowing.
Spinal cord tumors may cause numbness, weakness, or lack of coordination in the arms and/or legs (usually on both sides of the body), as well as bladder or bowel problems.
Having one or more of the symptoms above does not mean that your child definitely has a brain or spinal cord tumor. All of these symptoms can have other causes. Still, if your child has any of these symptoms, especially if they don’t go away or get worse over time, see your child’s doctor so that the cause can be found and treated, if needed.
Diagnosed
Brain and spinal cord tumors are usually found because of signs or symptoms a child is having. If a tumor is suspected, tests will be needed to confirm the diagnosis.
Medical history and physical exam
If your child has symptoms that suggest a brain or spinal cord tumor, the doctor will get a complete medical history, focusing on the symptoms and when they began. The doctor will also do a neurologic exam to check your child’s brain and spinal cord function, if possible. Depending on the child’s age, the exam may test reflexes, sensation, muscle strength, vision, eye and mouth movement, coordination, balance, alertness, and other functions.
If the results are abnormal, your child’s doctor may refer you to a neurologist (a doctor specializing in medical treatment of nervous system diseases) or a neurosurgeon (a surgeon specializing in nervous system diseases), who will do a more detailed exam and might order other tests.
Imaging tests
Your child’s doctors may order one or more imaging tests. These tests use x-rays, strong magnets, or radioactive substances to create pictures of internal organs such as the brain and spinal cord. The pictures may be looked at by doctors specializing in this field (neurosurgeons, neurologists, and neuroradiologists) as well as by your child’s primary care doctor.
Magnetic resonance imaging (MRI) and computed tomography (CT) scans are used most often for brain diseases. These scans will show a brain or spinal cord tumor, if one is present, in almost all cases. Doctors can often also get an idea about what type of tumor it might be, based on how it looks on the scan and where it is in the brain (or spinal cord).
Magnetic resonance imaging (MRI) scan
MRI scans are very good for looking at the brain and spinal cord and are considered the best way to look for tumors in these areas. MRI images are usually more detailed than those from CT scans (described below). But they do not image the bones of the skull as well as CT scans and therefore might not show the effects of tumors on the skull. MRI scans create detailed images using radio waves and strong magnets instead of x-rays, so they do not expose the child to radiation. A contrast material called gadolinium may be injected into a vein before the scan to help see details better.
MRI scans can take a long time – often up to an hour. Your child may have to lie on a table that slides inside a narrow tube, which is confining and can be distressing. The test also requires a person to stay still for several minutes at a time. Some children might need medicine to help them relax or even be asleep during the test. Open MRI machines may be another option, though they might result in less detailed images. The MRI machine makes loud buzzing and clicking noises that your child may find disturbing. Some places provide headphones or earplugs to help block this noise out.
Magnetic resonance angiography (MRA): This special form of MRI may be done to look at the blood vessels in the brain. This can be very useful before surgery to help the surgeon plan an operation.
Magnetic resonance spectroscopy (MRS): This test is like an MRI, except it measures the radio wave interactions with different chemicals in the brain. MRS highlights some features of brain tumors that may not be seen clearly with MRI. It creates graph-like results called spectra (but crude images can also be created). This might give clues to the type of tumor, but in most cases a biopsy of the tumor is still needed to get an accurate diagnosis. MRS can also be used after treatment to help determine if an area that still looks abnormal on another test is remaining tumor or if it is more likely to be scar tissue. Magnetic resonance perfusion: For this test, also known as perfusion MRI, a contrast dye is injected quickly into a vein. A special type of MR image is then obtained to look at the amount of blood going through different parts of the brain and tumor. Tumors often have a bigger blood supply than normal areas of the brain. A faster growing tumor may need more blood.
Perfusion MRI can give doctors an idea of the best place to take a biopsy. It can also be used after treatment to help determine if an area that still looks abnormal is remaining tumor or if it is more likely to be scar tissue.
Functional MRI (fMRI): This newer type of MRI looks for tiny blood flow changes in an active part of the brain. It can be used to determine what part of the brain handles a function such as speech, thought, sensation, or movement. Doctors can use this to determine which parts of the brain to avoid when planning surgery or radiation therapy.
This test is similar to a standard MRI, except that your child will be asked to perform specific tasks (such as answering simple questions or moving their fingers) while the scans are being done.
Computed tomography (CT) scan
The CT scan uses x-rays to produce detailed cross-sectional images of your child’s brain and spinal cord. Instead of taking one picture, like a regular x-ray, a CT scanner takes many pictures as it rotates around your child while he or she lies on a table. A computer then combines these pictures into images of slices of the body. Unlike a regular x-ray, a CT scan creates detailed images of the soft tissues in the body.
For brain and spinal cord tumors, CT scans are not used as often as MRI scans, which give slightly more detailed images and do not use radiation. Still, there are instances where CT scans may have advantages over MRI scans:
CT scans take much less time than MRIs, which can be particularly helpful for children who have trouble staying still.
CT scans provide greater detail of the bone structures near the tumor than MRIs do.
CT angiography (CTA), which is described below, can provide better details of the blood vessels in and around a tumor than MRA in some cases.
Before the scan, your child may get an injection of a contrast dye through an IV (intravenous) line. This helps better outline any tumors that are present. The contrast contains iodine and may cause some flushing (a feeling of warmth, especially in the face). Some people are allergic to the dye and get hives. Rarely, more serious reactions like trouble breathing or low blood pressure can occur. Be sure to tell the doctor if your child has any allergies or has ever had a reaction to any contrast material used for an imaging test.
CT angiography (CTA): For this test, your child gets an injection of contrast material through an IV line while he or she is in the CT scanner. The scan creates detailed images of the blood vessels in the brain, which can help doctors plan surgery. CT angiography can provide better details of the blood vessels in and around a tumor than MR angiography in some cases.
Positron emission tomography (PET) scan
For this test, a radioactive substance (usually a type of sugar known as FDG) is injected into the blood. The amount of radioactivity used is very low and passes out of the body within a day or so. Because tumor cells in the body are growing quickly, they absorb larger amounts of the sugar than most other cells. After about an hour, your child is moved onto a table in the PET scanner. He or she will lie on the table for about 30 minutes while a special camera creates a picture of areas of radioactivity in the body. If your child is not able to stay still for the test, this might require sedation.
The PET scan image is not as detailed as a CT or MRI scan, but it can provide helpful information about whether abnormal areas seen on other tests (such as MRIs) are likely to be tumors or not.
This test is also useful after treatment to help determine if an area that still looks abnormal on an MRI scan is remaining tumor or if it is more likely to be scar tissue. Any remaining tumor will show up on the PET scan, while scar tissue will not.
Angiogram
For this test, a special dye is injected into blood vessels near the tumor, and then the area is viewed with x-rays. This helps doctors look at a tumor’s blood supply. This test is not done much for brain or spinal cord tumors anymore, as it has largely been replaced by magnetic resonance angiography (MRA) or computerized tomographic angiography (CTA).
Brain or spinal cord tumor biopsy
Imaging tests such as MRI and CT scans may show that a child has a brain or spinal cord tumor. But usually the type of tumor can be determined only by removing a sample of it, which is called a biopsy. A biopsy may be done as a procedure on its own for diagnosis, or it may be part of surgery to treat the tumor.
The biopsy samples are looked at under a microscope by a pathologist (a doctor specializing in diagnosis of diseases by lab tests). Sometimes it might need to be looked at by a neuropathologist, a pathologist who specializes in nervous system diseases. The pathologist determines if the tumor is benign or malignant (cancerous) and exactly what type of tumor it is.
In some cases (such as for many astrocytomas or brain stem gliomas), it may not be necessary or possible to biopsy the tumor safely, so the diagnosis is made based only on how the tumor looks on imaging tests. Biopsies can be done in different ways.
Stereotactic needle biopsy
This type of biopsy may be used if imaging tests show surgery to remove the tumor might be too risky (such as with some tumors in vital areas or deep within the brain) but a sample is still needed to make a diagnosis.
Depending on the situation, the biopsy may be done with the child awake or under general anesthesia (asleep). If the child is awake, the neurosurgeon injects a local anesthetic into areas of skin over the skull to numb them. (The skull and brain itself do not feel pain.)
A rigid frame may then be attached onto the child’s head. This helps make sure the surgeon will target the tumor precisely. A small cut is made in the scalp, and a small hole is drilled in the skull. An MRI or CT scan is used along with the frame to help the neurosurgeon guide a hollow needle into the tumor to remove small pieces of tissue. Another approach is to get an MRI or CT scan, use scalp markers or facial and scalp contours to create a map of the inside of the head, and then use an image-guidance system to direct the needle into the tumor. This still requires making an incision and drilling a small hole into the skull.
The biopsy samples are then looked at under a microscope by a pathologist. The doctor can usually tell exactly what type of tumor it is. This helps determine the best course of treatment and the prognosis (outlook).
Craniotomy
If imaging tests show the tumor can be treated with surgery, the neurosurgeon may not do a needle biopsy. Instead, he or she may do an operation called a craniotomy (described in the Surgery section) to remove all or most of the tumor. (Removing most of the tumor is known as debulking.)
Small samples of the tumor are looked at right away by the pathologist while the child is still in the operating room, to get a preliminary diagnosis. This can help guide treatment, including whether further surgery should be done at that time. A final diagnosis is made a within a few days in most cases.
You can read more about the kinds of tests that are done on biopsy or tissue samples in Testing Biopsy and Cytology Specimens for Cancer.
Lumbar puncture (spinal tap)
This test is used to look for cancer cells or chemicals released by tumors in the cerebrospinal fluid (CSF), which is the liquid that bathes the brain and spinal cord. For this test, the doctor first numbs an area in the lower part of the back over the spine. The doctor may also recommend that the child be given something to make them sleep so the lumbar puncture can be done more easily and safely. A small, hollow needle is then placed between the bones of the spine to withdraw some of the fluid.
The fluid is looked at under a microscope for cancer cells. The CSF can also be tested for certain substances released by some germ cell tumors.
Lumbar punctures are often used if a tumor has already been diagnosed as a type (such as a medulloblastoma) that can commonly spread through the CSF. Information from the spinal tap can influence treatment.
Bone marrow aspiration and biopsy
Because some tumors (especially medulloblastomas) can spread beyond the nervous system, in some instances the doctor may recommend looking at cells in your child’s bone marrow (the soft, inner part of certain bones) to see if tumor cells have spread there.
The bone marrow aspiration and biopsy are often done at the same time. The samples are usually taken from the back of the pelvic (hip) bone, but in some cases they may be taken from other bones.
In bone marrow aspiration, the skin over the hip and the surface of the bone is cleaned and then numbed with local anesthetic. In most cases, the child is also given other medicines to make them drowsy or even asleep during the procedure. A thin, hollow needle is then inserted into the bone, and a syringe is used to suck out (aspirate) a small amount of liquid bone marrow. A bone marrow biopsy is usually done just after the aspiration. A small piece of bone and marrow is removed with a slightly larger needle that is pushed down into the bone. Once the biopsy is done, pressure is applied to the site to help stop any bleeding
The specimens are then looked at under a microscope for tumor cells.
Blood and urine tests
These lab tests are rarely used to diagnose brain and spinal cord tumors, but if your child has been sick for some time they may be done to check how well the liver, kidneys, and some other organs are working. This is especially important before any planned surgery.
If your child is getting chemotherapy, blood tests will be done routinely to check blood counts and to see if the treatment is affecting other parts of the body.
For More Information Visit Us Our Website: https://www.healthinfi.com
0 200
No Comments